
TL/DR
Statins are medicines that lower bad cholesterol levels in the blood. They are essential for heart health but may cause muscle discomfort. Geranylgeraniol (GG) supports mitochondrial function and promotes healthier muscle performance, making long-term statin use more comfortable and sustainable.
Statins are medications that reduce cholesterol production in the body that are widely used for primary and secondary prevention of cardiovascular diseases (heart attack, stroke, atherosclerotic disease).
They work by lowering LDL (low-density lipoprotein, also known as bad cholesterol), which reduces the risk of atherosclerosis (fatty deposits that narrow blood vessels). Moreover, they also block HMG-CoA reductase, the rate-limiting enzyme in the liver’s cholesterol biosynthesis pathway
However, due to prolonged use of statins, some individuals may gradually notice mild muscle discomfort over time. These effects, ranging from mild soreness to a sense of muscle heaviness, are clinically grouped as statin-associated muscle symptoms (SAMS).
While not everyone experiences them, understanding SAMS offers a more balanced and realistic view of long-term statin use in everyday life. Let’s begin by understanding how statin works.
Statins: How Do They Work
The clinical impact of statins can be best understood by examining their dual action on cholesterol metabolism and the mevalonate pathway.
Statins work by blocking the liver’s cholesterol production, reducing cardiovascular disease risk and offering additional anti-inflammatory and vascular-protective benefits.
1. Cholesterol-Lowering Effect
Statins block HMG-CoA Reductase (3-Hydroxy-3-Methylglutaryl-Coenzyme A) in the liver, reducing cholesterol production. This drop in intracellular cholesterol signals liver cells to increase LDL receptor expression, pulling more LDL (“bad”) cholesterol from the bloodstream. As a result, statins lower LDL levels by 20–60% and significantly reduce cardiovascular risk.
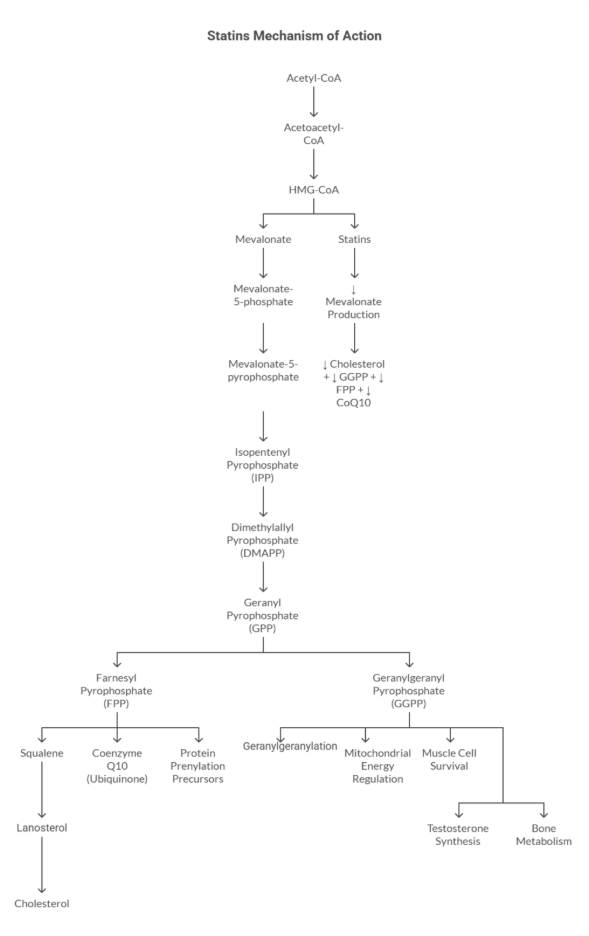
2. Mevalonate Pathway Effect
- HMG-CoA reductase is also a key enzyme in the mevalonate pathway that functions primarily in the liver cells.
- Important by-products of this pathway include:
- Cholesterol: essential for the formation of cell membranes and the synthesis of hormones.
- Coenzyme Q10 (CoQ10 or ubiquinone): essential for mitochondrial energy production
- Isoprenoid intermediates such as farnesyl pyrophosphate (FPP), geranylgeranyl pyrophosphate (GGPP), and geranylgeraniol (GG), which support cellular signaling and survival.(1)
- Reduction of HMG-CoA into mevalonate is an essential rate-limiting step in cholesterol production.
- The rate-limiting step means it controls the overall speed of the entire pathway.
How Statins Interrupt the Mevalonate Pathway
- Statins inhibit HMG-CoA reductase, the rate-limiting enzyme of the mevalonate pathway, reducing mevalonate production at its source.
- This slowdown lowers downstream by-products, including cholesterol, CoQ10, GGPP, and GG, and limits protein prenylation.
- As a result, key processes such as cell repair, mitochondrial energy production, muscle signaling, and anti-inflammatory balance are affected.
- Over time, GGPP depletion may contribute to muscle pain, weakness, and exercise intolerance, collectively referred to as statin-associated muscle symptoms (SAMS).
Let’s take a closer look at what SAMS really means and why it matters.
Understanding Statin Associated Muscle Symptoms (SAMS)
- Statin-associated muscle symptoms refer to any muscle-related discomfort that appears while a person is on long term statin medication.
- These symptoms can manifest as muscle aches, soreness, stiffness, tenderness, cramps, fatigue, and rarely as prolonged weakness.
- Understanding SAMS is critical, as it is the leading cause of statin discontinuation, increasing the risk of heart attack, stroke, and cardiovascular death.
- SAMS affects about 1 in 10 people taking statins, although reports range from 5–25%. Muscle symptoms directly caused by statins are far less common, occurring in only 1–2% of users.
Typical Muscle Symptoms Linked to Statins
Most people who experience muscle symptoms with statins notice:
- Pain or soreness on both sides of the body.
- Discomfort in the thighs, calves, or upper arms.
- Symptoms starting 4–8 weeks after beginning or increasing statin.
- Normal or slightly high creatine kinase(CK) levels on blood tests.
- Serious muscle damage is very rare.(2)
Who is at Higher Risk?
- Older adults
- High-dose statin users
- Individuals with vitamin D deficiency
- People with hypothyroidism, diabetes, or high physical activity
- Drug interactions affecting statin metabolism
Now that we have explored SAMS, the next step is to examine clinical studies and understand how these symptoms can be prevented.
Clinical Evidence: What Research Shows about Statin-Associated Muscle Symptoms (SAMS)Prevention
SAMS becomes clearer when viewed through clinical data, which also highlights how these symptoms can be prevented. Over the past decade, researchers have conducted randomized trials, mechanistic experiments, and large meta-analyses to uncover why muscle symptoms occur, how often they are truly caused by statins, and what strategies help patients stay on therapy. Let’s take a look at it.
Clinical Evidence Table: Statin Associated Muscle Symptoms (SAMS) Prevention Studies
| Study / Year | Design | N | Population | Dose / Intervention | Duration | Key Result |
| STATIN WISE, 2021(3) | N-of-1 Randomized, Placebo-Controlled | 151 | Patients with previous SAMS | Atorvastatin 20 mg vs placebo | 12 months | Muscle symptoms did not differ between statin and placebo. It showed strong nocebo effect (feeling symptoms because you expect them) |
| SAMSON, 2021(4) | N-of-1 Randomized | 60 | Individuals who recently stopped statins due to SAMS | Statin vs placebo vs empty pill bottle | 12 months | 90% of symptoms also occurred on placebo; many patients restarted statins after trial. |
| STOMP, 2013(5) | RCT | 420 | Statin-naïve adults | Atorvastatin 80 mg | 6 months | Small increase in muscle pain and CK; no change in strength or exercise performance. |
| CTT Meta-analysis, 2022(6) | Meta-analysis of 23 RCTs | 154,664 | General statin users | All statins (various doses) | Up to 5 years | <1% true pharmacologic SAMS; most symptoms not caused by statins. |
| CoQ10 Trials (Meta-analyses)(7) | Multiple RCTs | ~800 total | SAMS patients | CoQ10 (100–600 mg/day) | 4–12 weeks | Mixed results, some show reduced pain, others no difference. |
| Vitamin D RCTs (VITAL Substudies)(8) | RCT | >2,000 | Individuals with & without deficiency | Vitamin D 2000 IU/day | 2–4 years | Did not reduce SAMS incidence or severity; benefit only possible in severe deficiency. |
| RACING Trial, 2022(9) | RCT | 3,780 | ASCVD patients | Rosuvastatin 10 mg + ezetimibe vs rosuvastatin 20 mg | 3 years | Combination therapy improved statin tolerability & LDL-C target achievement. |
| Statin Switching Cohorts(10) | Observational | ~1,000 | SAMS patients switching statins | Pravastatin or rosuvastatin | Variable | Hydrophilic statins associated with fewer muscle symptoms. |
Overall, high-quality trials show that true pharmacologic SAMS is uncommon (<1–2%), with most muscle symptoms explained by a nocebo effect (muscle symptoms triggered by worry or expectation, not the statin itself) rather than statin toxicity.
Strategies such as dose adjustment, statin switching, or combination therapy can improve tolerability while preserving LDL-lowering benefits.
After examining what clinical studies reveal about SAMS, it’s important to look beyond symptoms and understand the underlying biochemistry. This is where a naturally occurring compound Geranylgeraniol (GG) comes into focus. Let’s understand what GG is and its relation to long term statin use.
What is Geranylgeraniol (GG)
Geranylgeraniol (GG or GGOH) is a naturally occurring diterpene alcohol produced endogenously via the mevalonate pathway—the same metabolic route that generates cholesterol, Coenzyme Q10 (CoQ10), vitamin K2, and other isoprenoid-derived compounds.(11) Functionally, GG supports:
- Mitochondrial energy production, by helping maintain CoQ10 synthesis, which is vital for electron transport chain function.
- Hormone synthesis, including testosterone production in Leydig cells.
Also Read: Is your supplement missing an important ingredient: Geranylgeraniol
GG as a Precursor to an Essential Molecule (GGPP)
- Inside the body, GG is converted into geranylgeranyl pyrophosphate (GGPP) through mevalonate pathway to keep cells functioning normally.
- GGPP is required to activate various GTP binding proteins which help in cell growth, muscle repair, and mitochondrial energy output. Without GTP-binding, these proteins stay inactive, leading to impaired cellular function.(12)
Also Read: The Potential of Geranylgeraniol in Lowering Cholesterol
Geranylgeraniol (GG) as Major Player in Muscle Health and Energy Production
- Geranylgeraniol (GG) acts as a precursor to Geranylgeranyl pyrophosphate (GGPP), which anchors important proteins to cell membranes and supports muscle function and calcium balance.
- GG helps mitochondria in maintenance of ATP (energy) production and lower oxidative stress.(11)
Muscles especially cardiac(heart) and large skeletal muscles depend entirely on mitochondria, so GGPP is crucial for their performance and recovery
GG As Regulator of Inflammation and Antioxidant Pathways
It is seen that GG influences NF-kB (inflammation control), antioxidant enzymes and cell survival pathways, thereby preventing muscle breakdown from metabolic or oxidative stress.
Geranylgeraniol (GG) and Statin Associated Muscle Symptoms (SAMS)
Statins block HMG-CoA reductase, the enzyme at the start of the mevalonate pathway.
This reduces cholesterol, which is definitely a good sign, but it also lowers GGPP and CoQ10, which can affect muscle function in some individuals.
As GGPP drops, it might lead to the development of Statin-Associated Muscle Symptoms
Long-term statin use → reduced GGPP → impaired protein prenylation → mitochondrial dysfunction → increased oxidative stress → SAMS
However, taking GG supplementation can work wonders.
Also Read: Geranylgeraniol and Statins: What to know about GG as an alternative to GG Side-Effects
Early human studies show that GG is safe and well-tolerated. To make things clearer, let’s look at a summary of the key studies that link GG, muscle health, and statin use(11)
Geranylgeraniol (GG) and Statin Research Summary Table
| Study / Year | Design | N | Population / Model | Dose / Intervention | Key Result |
| Jiwan et al., 2022(13) | In-vivo | Rodents | Diabetic skeletal muscle degeneration model | Oral GG | Improved mitochondrial quality, enhanced autophagy, and prevented muscle degeneration. |
| Shirakawa et al. 2021(14) | In-vivo | Rodents | Oral frailty / muscle atrophy affecting chewing & speech | Oral GG | Reversed oral muscle atrophy and improved muscle function. |
| Sanvee et al., 2021(15) | Mechanistic review + experimental evidence | — | Human cells & animal models | GG rescue mechanisms | GG restored CoQ10, reduced statin myotoxicity, improved mitochondrial function. |
| Irwin et al., 2020(16) | In-vivo | Rodents | Statin-induced muscle fatigue model | Oral GG | Prevented muscle fatigue; improved force production and endurance. |
| Miyawaki et al., 2020(17) | In-vivo | Rodents | Denervation-induced skeletal muscle atrophy | GG supplementation | Preserved muscle fiber size and prevented atrophy progression. |
| Matsubara et al., 2018(18) | In-vitro | Cell study | Skeletal muscle cells | GG supplementation | Increased myogenic differentiation; reduced muscle atrophy markers (atrogin-1, MuRF1). |
| Irwin et al., 2018(19) | In-vivo | Rodents | Statin-induced muscle atrophy model | Oral GG | Increased muscle force; reduced atrogin-1; improved muscle integrity. |
| Schumacher et al., 2015(20) | Molecular enzymatic study | — | UBIAD1 pathway (vitamin K pathway) | GG–UBIAD1 interaction | Identified GG as required for MK-4 (menaquinone-4) synthesis → supports musculoskeletal health. |
| Campia et al., 2009(21) | In-vitro | Cell study | Monocytic cells exposed to statins | GG supplementation | Restored mitochondrial respiration; suggested role in CoQ10 regeneration. |
| Cao et al., 2009(22) | In-vitro & Animal | Various | Statin-treated myocytes & rodents | GG rescue treatment | Completely reversed statin-induced myofiber loss; reduced atrogin-1 by ~65%. |
| Johnson et al., 2004(23) | In-vitro mechanistic | Cell study | Statin-induced toxicity | GG supplementation | Demonstrated that statins block GG synthesis → impaired prenylation → muscle toxicity. |
| Raiteri et al., 1997(24) | Mechanistic case-series | — | Statin-induced rhabdomyolysis | — | Identified GG depletion—not cholesterol—as a cause of severe muscle breakdown. |
To sum up, preclinical evidence indicates that GG supplementation improves mitochondrial health and muscle integrity in models of statin-associated muscle stress. This supports further investigation of GG as a nutritional strategy targeting mevalonate pathway related muscle dysfunction.
Limitations of Current Evidence
- Many muscle symptoms happen even with placebo (a dummy treatment with no active drug), so it’s hard to know which are truly caused by statins.
- Human studies on GG are still missing as most evidence comes from animals and cell models.
- Different types of statins may have varying effects on muscle health, yet many studies do not clearly compare these differences.
- High-risk groups (older adults, women, diabetics) are not well represented in trials.
- Muscle pain is usually self-reported, which can be subjective.
Conclusion
Although uncommon, true SAMS may be associated with reduced levels of Geranylgeraniol (GG). Incorporating GG can be a practical way to support muscle health and improve overall statin tolerance, allowing individuals to enjoy the heart-protective benefits of statins with greater ease.
Key takeaways
- Statins lower cholesterol effectively and remain essential for long-term heart health.
- Statins reduce not only cholesterol but also important compounds like GGPP and CoQ10, which support muscle energy.
- Geranylgeraniol (GG) helps restore the mevalonate pathway and supports healthier muscle function.
- GG promotes better mitochondrial energy production and reduces oxidative stress in muscle cells.
- Supporting muscle health with GG allows people to enjoy the cardiovascular benefits of statins with improved ease and confidence.
FAQ’s
Statin-associated muscle symptoms (SAMS) typically involve mild, symmetrical muscle aches, soreness, weakness, or fatigue, often with normal blood tests.
Statins may lower muscle-supporting molecules like GGPP and CoQ10, and factors such as age, activity level, and drug interactions can increase susceptibility.
No, speak to your doctor. Often, the dose, type of statin, or timing can be adjusted safely.
Animal studies suggest Geranylgeraniol is safe and may reduce muscle problems, but human studies are still needed.
Animal and cell studies show GG supports muscle force, recovery, and mitochondrial performance, suggesting potential for improved muscle function.
References
- McFarland AJ, Anoopkumar-Dukie S, Arora DS, Grant GD, McDermott CM, Perkins AV, Davey AK. Molecular mechanisms underlying the effects of statins in the central nervous system. Int J Mol Sci. 2014;15(11):20607–20637. doi:10.3390/ijms151120607. PMID: 25391045; PMCID: PMC4264186.
- Warden BA, Guyton JR, Kovacs AC, et al. Assessment and management of statin-associated muscle symptoms (SAMS): A clinical perspective from the National Lipid Association. J Clin Lipidol. 2023;17(1):19-39. doi:10.1016/j.jacl.2022.09.001
- Herrett E, Williamson E, Brack K, et al. Statin treatment and muscle symptoms: series of randomised, placebo controlled n-of-1 trials. BMJ. 2021;372:n135.
- Howard JP, Wood FA, Finegold JA, et al. Side effect patterns in a crossover trial of statin, placebo, and no treatment. J Am Coll Cardiol. 2021;78(12):1210-1222.
- Parker BA, Capizzi JA, Grimaldi AS, et al. Effect of statins on skeletal muscle function. Circulation. 2013;127(1):96-103.
- Cholesterol Treatment Trialists’ Collaboration. Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022;400(10360):832-845.
- Qu H, Guo M, Chai H, Wang WT, Gao ZY, Shi DZ. Effects of Coenzyme Q10 on statin-induced myopathy: an updated meta-analysis of randomized controlled trials. J Am Heart Assoc. 2018;7(19):e009835.
- Manson JE, Cook NR, Lee IM, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380:33-44. (VITAL Trial includes muscle symptom analyses)
- Kim BK, Hong SJ, Lee YJ, et al. Long-term efficacy and safety of moderate-intensity statin with ezetimibe combination therapy versus high-intensity statin monotherapy in patients with atherosclerotic cardiovascular disease (RACING). Lancet. 2022;400(10354):380-392.
- Bruckert E, Hayem G, Dejager S, Yau C, Bégaud B. Mild to moderate muscular symptoms with high-dosage statin therapy—the PRIMO study. Cardiovasc Drugs Ther. 2005;19(6):403-414. (Supports statin switching evidence)
- Tan BK, Chin KY. Potential role of geranylgeraniol in managing statin-associated muscle symptoms: a COVID-19 related perspective. Front Physiol. 2023;14:1246589. doi:10.3389/fphys.2023.1246589. eCollection 2023.
- Muehlebach ME, Holstein SA. Geranylgeranyl diphosphate synthase: Role in human health, disease and potential therapeutic target. Clin Transl Med. 2023;13(1):e1167. doi:10.1002/ctm2.1167.
- Jiwan R, Ohno Y, Maekawa M, et al. Geranylgeraniol improves mitochondrial quality and alleviates skeletal muscle degeneration in diabetic mice. Nutrients. 2022;14(5):1010.
- Shirakawa T, Kimira M, Tanaka T, et al. Oral geranylgeraniol reverses skeletal muscle atrophy associated with oral frailty. Nutrients. 2021;13(11):3848
- Sanvee GM, Panajatovic MV, Lerch M, et al. Mechanisms of statin-associated myopathy: emerging biomarkers and therapeutic strategies. Pharmacol Ther. 2021;217:107663
- Irwin R, Lin H, Owens JA, et al. Geranylgeraniol prevents statin-induced muscle fatigue and improves muscle force production. J Cachexia Sarcopenia Muscle. 2020;11(2):447-461.
- Miyawaki K, Miyake M, Nomura K, et al. Geranylgeraniol prevents denervation-induced skeletal muscle atrophy. J Physiol Sci. 2020;70(1):32
- Matsubara T, Naruse K, Arakawa T, et al. Geranylgeranyl-pyrophosphate promotes myogenic differentiation and suppresses muscle atrophy-related ubiquitin ligases. Biochem Biophys Res Commun. 2018;495(1):1449-1455
- Irwin R, Lee J, Owens JA, et al. Geranylgeraniol increases muscle force output and protects against statin toxicity. J Cachexia Sarcopenia Muscle. 2018;9(4):788-802.
- Schumacher MM, Elsabrouty R, Seemann J, et al. The UBIAD1 prenyltransferase links intracellular cholesterol transport to vitamin K metabolism. Cell Metab. 2015;21(5):758-770.
- Campia I, Gamba P, Panzalorto M, et al. Statins impair mitochondrial respiration in human monocytic cells: protective role of geranylgeraniol. Atherosclerosis. 2009;203(2):429-438.
- Johnson TE, Zhang X, Bleicher KB, et al. Statins induce muscle damage by inhibiting geranylgeranyl pyrophosphate synthesis. Toxicol Appl Pharmacol. 2004;200(3):192-200.
- Raiteri M, Granata A, Lugli F, et al. Mevalonate pathway intermediates and statin-induced rhabdomyolysis. Pharmacol Res. 1997;35(4):301-307.