TL/DR: Testosterone levels naturally decline with age, leaving many men in a “low-T” range that doesn’t qualify for hormone therapy. A recent randomized, placebo-controlled clinical trial found that geranylgeraniol (GG) was safe and showed a few improvements in testosterone markers in men with lower baseline levels, showing GG as a promising, science-based support for better testosterone health.
Testosterone is the primary male hormone that supports energy levels, muscle strength, metabolic health, mood, and sexual function. However, testosterone levels in men naturally decline by approximately 1–2% per year after age 30. (1)
In Due to this, many men fall into a “low-T zone” in which testosterone levels may not be low enough to be considered a medical problem, but they are often lower than what men experienced in their younger years, typically around ~300–700 ng/dL. Men in this range may see few physical changes but they may not necessarily qualify for (TRT)
While TRT can restore hormone levels, it is not the first choice of interest as concerns surrounding fertility suppression, prostate monitoring, cardiovascular risk, and long-term dependence have prompted growing interest in non-hormonal, evidence-based alternatives.
Bhasin et al. reviewed clinical evidence on testosterone replacement therapy (TRT) in “Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline” and concluded that while TRT can improve muscle mass, bone density, and sexual function in men with confirmed androgen deficiency, it requires strict patient selection and ongoing monitoring.
The guideline highlights risks including polycythemia, prostate surveillance, fertility suppression, and potential cardiovascular effects, reinforcing that TRT is a medical therapy, not a routine wellness option.(2)
One such option gaining attention is geranylgeraniol (GG), a naturally occurring compound involved in cellular signaling. A recent clinical trial now explores whether GG can safely support healthy testosterone levels in men with lower baseline values without directly supplying hormones. Let’s learn how testosterone is produced.
From Production to Performance: Understanding Testosterone
Testosterone is the primary androgen hormone in men and is produced primarily in the Leydig cells of the testes (male reproductive organ). Its production is controlled by the hypothalamic–pituitary–gonadal (HPG) axis.
Males and females both naturally produce testosterone, though males have a higher production of testosterone.
In males, most testosterone is produced by the testes, whereas in females, testosterone is produced by the ovaries (female reproductive organ) in very small amounts and converted to female sex hormones.
The hormone is also produced in the adrenal glands of both males and females. (1)
Formation of Testosterone
Testosterone production follows a tightly regulated, stepwise process controlled by the brain and testes. Let’s understand it in a simpler way.
- The brain releases gonadotropin-releasing hormone (GnRH), which stimulates the pituitary gland to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH).
- LH travels through the bloodstream to the testes, where it activates Leydig cells to initiate testosterone synthesis
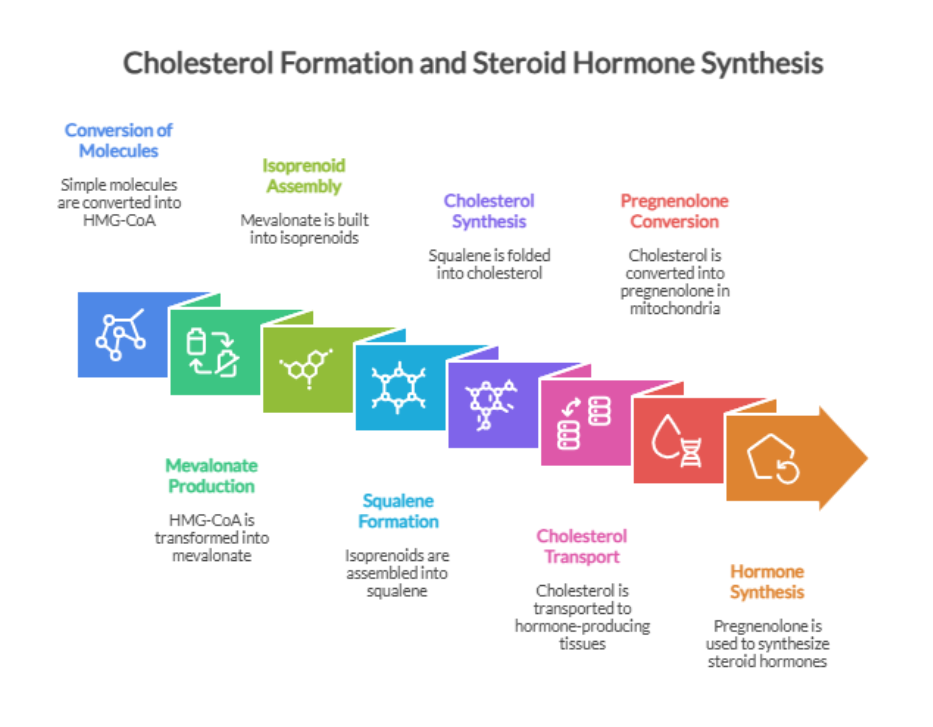
- Within these cells, cholesterol is converted to testosterone through several enzyme-driven steps that involve intermediates such as dehydroepiandrosterone (DHEA) and androstenedione.
- Once released, most testosterone circulates bound to proteins such as sex hormone–binding globulin (SHBG) and albumin, whereas a small fraction is available and exerts biological effects on muscle, bone, and reproductive tissues.
- Some testosterone is converted to more potent androgen dihydrotestosterone.
- As testosterone levels rise, the brain signals the body to slow down and maintain balanced hormone levels.(3)

Functions of Testosterone
Testosterone supports muscle, keeps bones strong, helps in the management of body fat, supports libido and sperm production, and influences mood, energy and motivation. Here is how:
- Muscle mass and strength
- Testosterone stimulates muscle protein synthesis and supports the growth and maintenance of lean muscle tissue. Low testosterone levels are associated with reduced muscle mass, strength loss, and increased risk of sarcopenia.
- Bone density
- Testosterone promotes bone formation and helps maintain bone mineral density throughout adulthood. Declining testosterone increases the risk of bone loss and fractures, especially as you age.
- Fat metabolism and insulin sensitivity
- Testosterone helps in the regulation of fat distribution and supports healthy insulin signaling. Lower levels are linked to increased abdomen fat, insulin resistance, and metabolic dysfunction.
- Libido and sperm production
- Testosterone is essential for normal erectile function. It also supports spermatogenesis by maintaining the proper function of the testes and reproductive tissues.
- Mood, energy, and motivation
- Adequate testosterone levels are associated with better mood stability, energy, and motivation. Low levels are commonly linked to fatigue, low drive, and depressive symptoms.(4)
What is the normal range of testosterone?
Normal total testosterone levels in healthy adult men range from 300–1,000 ng/dL (nanograms per deciliter), measured via morning blood tests. It declines 1-2% yearly after 30 due to reduced Leydig cell output. (5)
You will be surprised to know that testosterone production begins even before birth, reflecting how deeply this hormone is woven into the human life cycle. Levels rise through childhood and usually peak in the early 20’s (6)
From here, testosterone levels gradually decline as men age, though the rate of decline may vary with causes. The table below shows the reference ranges for normal testosterone levels by age in men and women. Although this range may vary according to the laboratory and Tanner stage in children.(7)
Normal testosterone levels by age in men and women
| Age | Men (nmol/L) | Women (nmol/L) |
| 2 to 10 | <0.24–0.35 | <0.24–0.41 |
| 11 to 15 | <0.24–26.25 | <0.24–0.96 |
| 16 to 17 | 7.92–27.0 | 0.41–1.50 |
| 18–49 | 8.7–29.0 | 0.29–1.67 |
| 50+ | 6.7–25.7 | 0.1–1.42 |
What happens when testosterone levels are lower than the body needs?
Testosterone acts like a messenger that supports many day-to-day functions. Whenever testosterone levels drop, hormone signaling begins to weaken. Low testosterone actually exists as a spectrum.
- At one end is clinical hypogonadism, a medical condition in which testosterone levels are consistently low and accompanied by clear symptoms such as severe fatigue, muscle loss, sexual dysfunction, or infertility. This form requires medical evaluation and, in many cases, hormone therapy.
- However, at the other end, there is a more common form in which men experience low testosterone (“low-T”) that does not meet medical criteria for hypogonadism.
In this gray zone, testosterone levels are lower than in earlier adulthood, typically within reference ranges of 300–700 ng/dL. Let’s discuss in detail below:(8)
Common Causes of Low T
- Aging: Testosterone levels naturally decline by about 1–2% per year after age 30.
- Excess body fat: Obesity can disrupt hormone signaling and increase testosterone conversion to estrogen.
- Poor sleep: Inadequate or irregular sleep reduces testosterone production.
- Chronic stress: High cortisol levels suppress testosterone synthesis.
- Metabolic conditions: Disorders such as type 2 diabetes and insulin resistance are linked to lower testosterone levels.(4)
The table below summarizes the key differences between normal testosterone levels, functional or “low-T”, and clinical hypogonadism, based on commonly used laboratory ranges, clinical guidelines, and research literature.
Normal Testosterone vs. Low Testosterone (“Low-T”) vs. Clinical Hypogonadism
| Category | Normal Testosterone Levels | Low Testosterone (“Low-T” Zone) | Clinical Hypogonadism |
| Definition | Testosterone levels appropriate for age with no hormone-related symptoms | Levels lower than a man’s youthful baseline but not medically deficient | A medical condition marked by consistently low testosterone with clinical symptoms |
| Typical Total Testosterone Levels | Approximately 300–1,000 ng/dL (lab-dependent) | Commonly ~300–700 ng/dL, varies by age and individual baseline | Usually <300 ng/dL (confirmed on repeat morning tests) |
| Diagnosis Status | No diagnosis | Descriptive, non-diagnostic term | Formal medical diagnosis |
| Common Symptoms | Normal energy, muscle strength, libido, and metabolic health | Mild fatigue, reduced muscle tone, increased fat, lower motivation or libido | Marked fatigue, muscle loss, erectile dysfunction, infertility, bone loss |
| Primary Causes | Healthy endocrine and metabolic function | Aging, metabolic changes, stress, sleep disruption, lifestyle factors | Testicular failure or impaired HPG axis signaling |
| Medical Treatment | None required | Typically not treated with TRT | Often treated with testosterone replacement therapy (TRT) |
| Role of Lifestyle & Nutrition | Maintenance and prevention | Primary strategy for support and improvement | Supportive alongside medical therapy |
| Research Focus | Healthy aging and prevention | Non-hormonal lifestyle and nutritional interventions | Endocrinology and hormone replacement outcomes |
Although treatment plans may vary by diagnosis, the focus is shifting from testosterone replacement toward restoring physiological hormone production. Rather than replacing testosterone directly, these strategies aim to restore the cellular and biochemical pathways that govern steroid formation. (8)
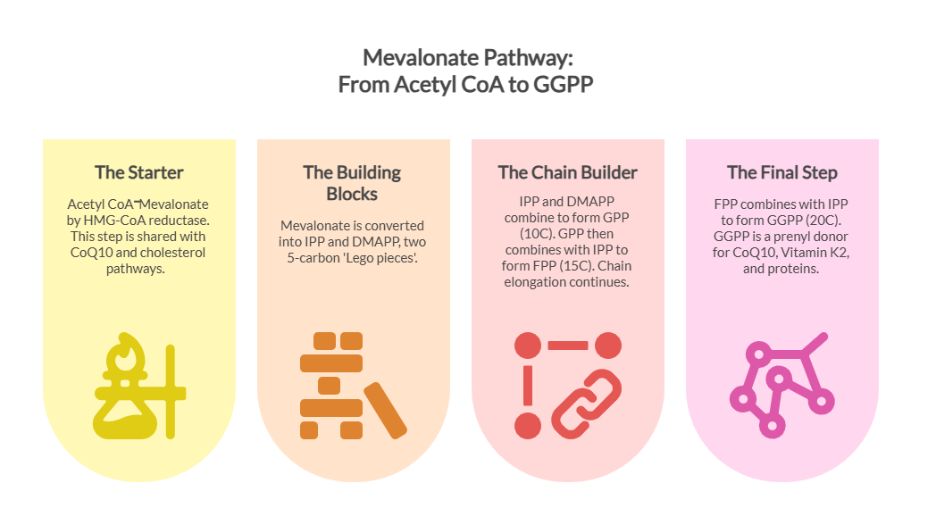
One such pathway is the mevalonate pathway product GG, which has emerged as a promising key molecule due to its role in supporting Leydig cell function and testosterone biosynthesis.
By replenishing a fundamental building block required for steroid hormone production, Geranylgeraniol represents a mechanistically distinct and potentially safer alternative for addressing age-related declines in testosterone.
What is Geranylgeraniol?
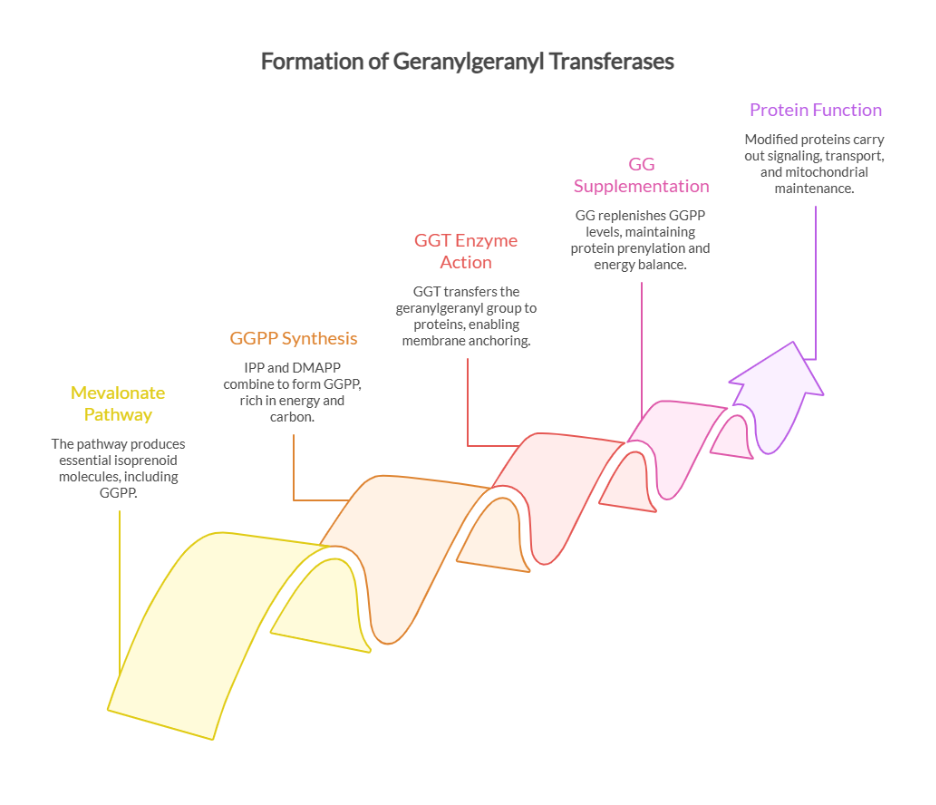
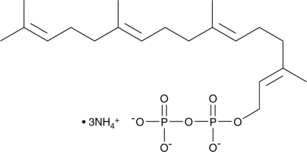
- Geranylgeraniol (GG) is a naturally occurring lipid molecule found in annatto ( Bixa orellana ) seeds. It is also synthesized endogenously in humans via the mevalonate pathway.
- It acts as a key precursor for essential biomolecules, including CoQ10, vitamin K2 (MK-4), and geranylgeranyl pyrophosphate (GGPP).
- GG plays a structural and regulatory role in cell signaling, mitochondrial function, and steroid hormone biosynthesis.
- However, endogenous GG levels may decline with aging, metabolic stress, or statin use, thereby interfering with the body’s endogenous hormone production.GG supplementation may therefore serve as a great strategy to restore the mevalonate pathway to support hormone synthesis. (9)
How GG Is Linked to Low Testosterone (Low T)
You might be surprised to learn that low testosterone isn’t always just a hormone issue, it’s often a pathway issue, as testosterone is made in Leydig cells through a process that depends on the mevalonate pathway. Geranylgeraniol (GG) also plays a critical role in the same pathway.
Low testosterone and mevalonate pathway insufficiency often reinforce one another. When the pathway slows, the biochemical support required for testosterone synthesis also declines.
Geranylgeraniol (GG) bridges this gap, complementing both sides by restoring a key pathway component that supports mitochondrial function and hormone production. Thereby, using the strength of one system to help correct the deficiency of the other.
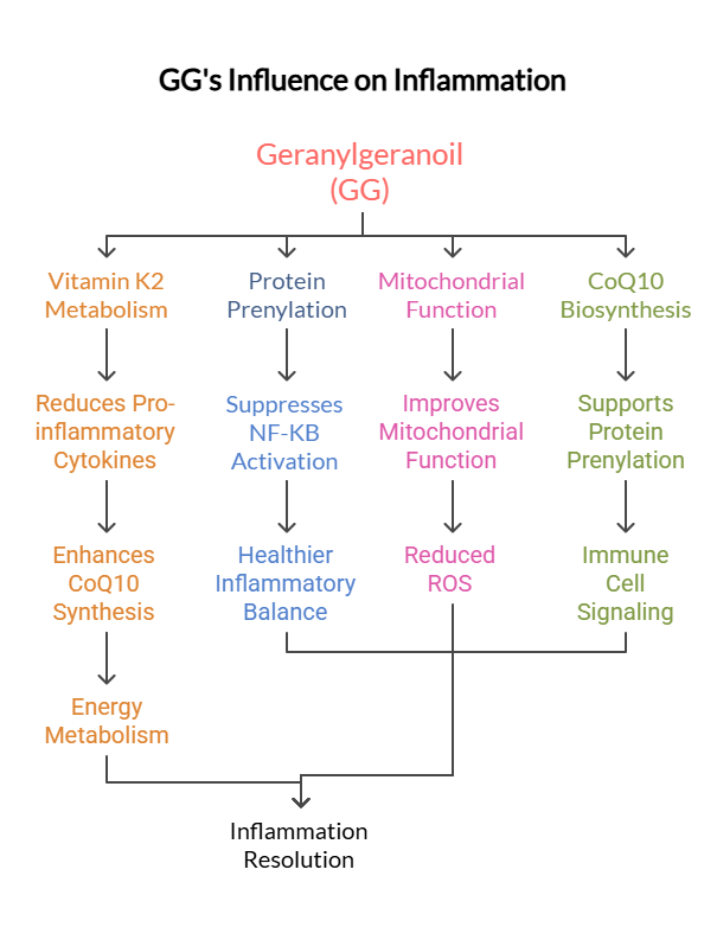
GG supports testosterone production by:
- Enhancing cholesterol transport into mitochondria, the first and rate-limiting step of steroidogenesis
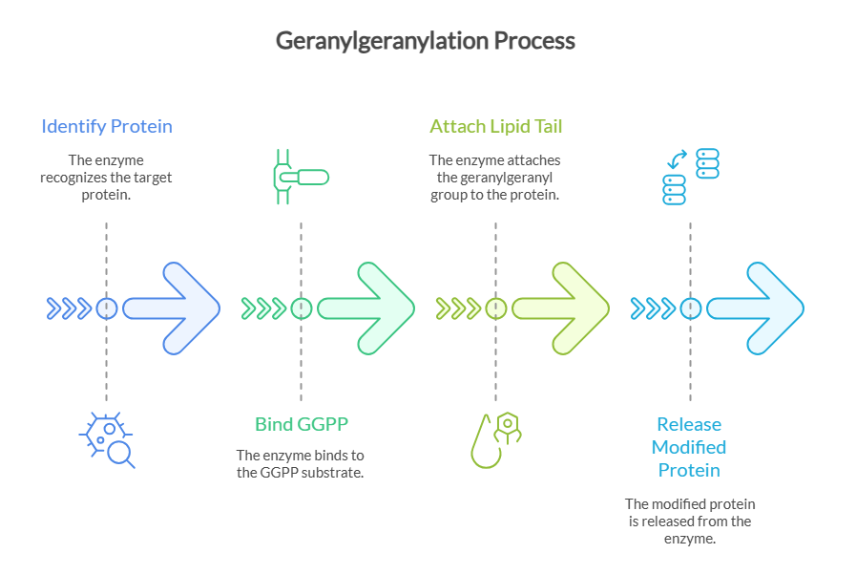
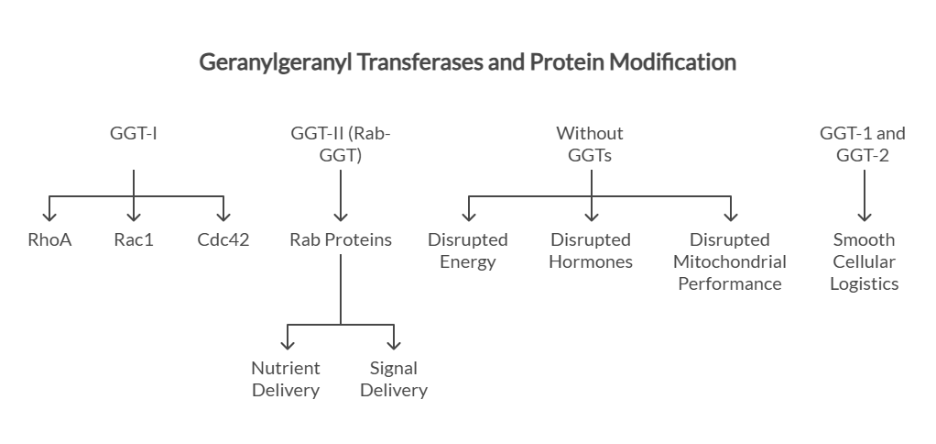
- Supporting prenylation of signaling proteins essential for LH/cAMP-mediated testosterone synthesis
- Maintaining mitochondrial energy efficiency, required for steroid hormone production. (9)
Building on this biological foundation, a recent randomized, double-blind, placebo-controlled clinical trial—The Effects of Geranylgeraniol on Blood Safety and Sex Hormone Profiles in Healthy Adults investigated whether GG supplementation could influence hormone profiles safely.(8)The study provides rare human data exploring GG’s potential role in supporting testosterone biology, particularly in men with lower baseline levels.
The Clinical Trial at a Glance
This study was conducted at the Applied Science and Performance Institute in Tampa, FL, USA, in accordance with all protocols to avoid bias. Let’s give you insights into the trial.
| Trial | Randomized, placebo-controlled, dose-escalated |
| Total Participants | 66 (Male and females) |
| Age Groups | 30-49 Years |
| Time Period | 8 weeks |
| Dose Escalation | 150 to 300 mg occurring every 4 weeks |
| Test Analysis | CBC (Complete Blood Count, Comprehensive Metabolic Panel, Progesterone, Estradiol, Testosterone |
| Testosterone Testing | Exploratory Analysis done in a subgroup of males with Baseline Testosterone <700ng/dL from pre-testing phase to 8 weeks Trial Randomized, placebo-controlled, dose-escalated Total Participants 66 (Male and females) Age Groups 30-49 Years Time Period 8 weeks Dose Escalation 150 to 300 mg occurring every 4 weeks Test Analysis CBC (Complete Blood Count, Comprehensive Metabolic Panel, Progesterone, Estradiol, Testosterone Testosterone Testing Exploratory Analysis done in a subgroup of males with Baseline Testosterone <700ng/dL from pre-testing phase to 8 weeks |
Study Design & Protocol
- A randomized, double-blind, placebo-controlled clinical trial, evaluated the short-term safety and hormonal effects of geranylgeraniol (GG). (8)
- The study used a dose-escalation design, providing 150 mg per day for the first four weeks followed by 300 mg per day for the next four weeks, for a total duration of eight weeks.
- Healthy adult men and women were enrolled, with primary selection criteria focused on blood chemistry, hematology, and sex hormone profiles.
Why are randomized, placebo-controlled trials done?
They are considered the gold standard for reducing bias and improving reliability
Materials and Methods
Participants received either Geranylgeraniol (GG) or a Visually Impaired Placebo. Let’s take a closer look at the ingredients that were included in both GG and placebo formulations.
| Geranylgeraniol (GG) Soft-Gel | Visually Impaired Placebo-PLA Supplement |
| Active Component- Geranylgeraniol (150mg) Inactive Components Bone Gelatin Purified Water Glycerin Carob in glycerin with caramel | Olive Oil Bone Gelatin Purified Water Carob in Glycerin with Caramel |
Methods
- Following baseline (Pre) testing, participants were assigned to either the GG or placebo (PLA) group. As the supplementation period was 8 weeks, it was divided into two phases (0-4 weeks and 5-8weeks).
- During the first 4 weeks, participants consumed two soft-gel capsules daily, one in the morning (AM) and one in the evening (PM), both with food.
- In the GG group, the AM capsule contained placebo and the PM capsule provided 150 mg of active GG (from 210 mg trans-geranylgeraniol, GG-Gold®)
- The PLA group received inactive capsules at both time points.
Here are the results:
After identical retesting at week 4, supplementation continued for an additional 4 weeks, during which the GG group consumed active GG in both AM and PM capsules for a total daily dose of 300 mg, whereas the PLA group continued placebo supplementation. Dose selection was based on human-equivalent dosing derived from prior animal studies.
All participants were retested 8 weeks later, and a supplement compliance assessment was done. It was observed that 96% in the GG group and 95% in the PLA group, with all analyzed participants demonstrating compliance greater than 80%.
GG GROUP
| Time | 0-4 Week | 5-8 Week |
| AM | Inactive Ingredient mimicking placebo PLA with food | 150 mg GG with food |
| PM | Active Geranylgeraniol- 150 mg from 210 Trans-GG Gold with food | 150 mg Geranylgeraniol (GG) with Food |
PLACEBO GROUP
| Time | 0-4 Week | 5-8 Week |
| AM | PLA with food | PLA with food |
Alongside, an exploratory analysis was performed to assess whether baseline testosterone levels influenced response to GG supplementation in which total, free, and bioavailable testosterone were measured at baseline (Pre), week 4 (Wk4), and week 8 (Wk8).
- For males, the normal total testosterone reference range (280–1100 ng/dL) was divided into quartiles. To focus on men with lower testosterone levels, participants with baseline total testosterone ≥700 ng/dL were excluded.
- Final male sample sizes consist of GG (n = 15) and PLA (n = 13). Statistical analysis was conducted across all time points and repeated for 0 week, 4 weeks, and 8 weeks.
Key Findings
- Across the full study population, the trial reported no significant changes in blood chemistry, hematology, or hormone safety markers, including estradiol, dihydrotestosterone (DHT), and sex hormone–binding globulin (SHBG).
- These findings indicate that GG supplementation was well tolerated over the eight-week study period and did not disrupt overall hormonal balance.
Low-Baseline Testosterone Subgroup
- In this subgroup, GG supplementation was associated with modest but statistically significant increases in total testosterone, free testosterone, and bioavailable testosterone.
- These effects were not observed in participants with higher baseline levels, highlighting the exploratory nature of this finding.
Biological Relevance of the Results
- Testosterone synthesis depends on steroidogenesis, a cellular process that converts cholesterol into testosterone within Leydig cells.
- Geranylgeraniol is not a hormone and does not directly stimulate testosterone release. Instead, mechanistic studies suggest GG supports the cellular signaling environment necessary for efficient steroid hormone production.
- This pathway-supportive role helps explain why testosterone increases were observed only in men with lower baseline levels and aligns with preclinical and cellular research findings.
Strengths of Evidence
- The trial’s randomized, double-blind, placebo-controlled design strengthens confidence in the data.
- The dosing protocol reflects real-world supplementation, and comprehensive blood safety monitoring supports short-term tolerability.
Limitations of Evidence
- The study was short in duration, and the testosterone findings emerged from a small exploratory subgroup rather than a primary endpoint.
- Additionally, the trial did not enroll men with diagnosed hypogonadism, limiting direct clinical application.
Key Takeaways from Study
- The findings suggest GG may be most relevant for men in the functional low-T range, rather than those with clinically diagnosed hypogonadism.
- These exploratory outcomes align with a study done by Ho et al., who reported an increase in testosterone levels in male rats supplemented with GG for 10 days at a dose of 48.3 mg/kg compared to rats on a control diet. (10)
- Because responses appear dependent on baseline testosterone levels, testing before supplementation is important.
- GG does not replace testosterone and should not be viewed as hormone therapy; instead, it may support endogenous production pathways.
Consultation with a healthcare professional remains essential when addressing hormone-related symptoms.
This study provides a foundational human data point, but further research is needed. Longer trials, inclusion of men with clinically low testosterone, and evaluation of functional parameters are needed to determine the broader relevance of GG in hormonal health. While the trial offers valuable insights, broader scientific validation comes from multiple independent studies. Let’s take a look at them.
| Study | Year | Design | Population | Dose | Duration | Key Results |
| Wilson et al (10) | 2020 | Preclinical (rodent) | Male rodents | GG supplementation | 4–12 weeks | ↑ Leydig cell steroidogenesis; restoration of mevalonate-dependent signaling |
| Sharpe et al.(11) | 2019 | Mechanistic cell/animal studies | Leydig cells / rodents | GG exposure | Variable | GG restored mitochondrial and prenylation pathways critical for steroid hormone synthesis |
| Lowery et al.(12) | 2014 | Preclinical (statin model) | Statin-treated rodents | GG co-administration | 6–8 weeks | GG prevented statin-induced suppression of steroidogenesis and muscle signaling |
Conclusion
Testosterone decline is a common part of aging, and for many men it falls into a functional low-T range rather than a medical deficiency. While testosterone replacement therapy is appropriate for diagnosed cases, growing interest lies in non-hormonal approaches that support natural hormone biology.
Early research on geranylgeraniol (GG) shows that it is safe to use in the short term and may help improve testosterone levels, especially in men who start with lower levels. While more long-term studies are still needed, GG appears to be a promising, science-backed option for men looking to support their testosterone naturally, without medications.
FAQs
Low testosterone is defined as total testosterone levels below 300ng/dL in adult men.
Supplements cannot replace medically necessary TRT, but quality supplements may support energy, muscle health, and overall wellness in men who do not meet criteria for hormone therapy.
Geranylgeraniol (GG) is a naturally occurring compound involved in cellular signaling pathways that support normal hormone production. It is not a hormone and does not act like testosterone.
Based on current evidence, Geranylgeraniol may be most relevant for men in the low-T gray zone, particularly those interested in non-pharmacological, wellness-focused approaches.
Yes. Resistance training, adequate sleep, weight management, stress reduction, and proper nutrition can support healthy testosterone levels naturally.
References
- Zirkin BR, Tenover JL. Aging and declining testosterone: past, present, and hopes for the future. J Androl. 2012;33(6):1111-1118. doi:10.2164/jandrol.112.017426
- Bhasin S, Cunningham GR, Hayes FJ, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536-2559. doi:10.1210/jc.2009-2354
- Nassar GN, Leslie SW. Physiology, testosterone. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated January 2, 2023.
- Kelly DM, Jones TH. Testosterone: a metabolic hormone in health and disease. J Endocrinol. 2013;217(3):R25–R45.
- Rojas-Zambrano JG, Rojas-Zambrano A, Rojas-Zambrano AF. Impact of testosterone on male health: a systematic review. Cureus. 2024;16(2):eXXXXX. PMCID: PMC12023631. PMID: 40290556.
- Scott, H., Mason, J. and Sharpe, R., 2009. Steroidogenesis in the Fetal Testis and Its Susceptibility to Disruption by Exogenous Compounds. Endocrine Reviews, 30(7), pp.883-925.
- Smith J. What is a normal testosterone level for your age? Reviewed by Rodgers S. Updated December 31, 2024.
- Gheith R, Sharp MGF, Stefan M, Ottinger C, Lowery R, Wilson J. The effects of geranylgeraniol on blood safety and sex hormone profiles in healthy adults: a dose-escalation, randomized, placebo-controlled trial. Nutraceuticals. 2023;3(4):605–618. doi:10.3390/nutraceuticals3040043
- Ho, H.-J. Shirakawa, H.; Giriwono, P.E.; Ito, A.; Komai, M. A Novel Function of Geranylgeraniol in Regulating Testosterone Production. Biosci. Biotechnol. Biochem. 2018, 82, 956–96.
- Ho HJ, Shirakawa H, Yoshida R, Ito A. Geranylgeraniol enhances testosterone production via the cAMP/protein kinase A pathway in testis-derived I-10 tumor cells. Biosci Biotechnol Biochem. 2016;80(4):–. doi:10.1080/09168451.2015.1123612
- Irwin JC, Fenning AS, Vella RK. Geranylgeraniol prevents statin-induced skeletal muscle fatigue without causing adverse effects in cardiac or vascular smooth muscle performance. Transl Res. 2020;215:17-30. doi:10.1016/j.trsl.2019.08.004:
- Jaśkiewicz A, Pająk B, Litwiniuk A, Urbańska K, Orzechowski A. Geranylgeraniol prevents statin-dependent myotoxicity in C2C12 muscle cells through RAP1 GTPase prenylation and cytoprotective autophagy. Oxid Med Cell Longev. 2018;2018:6463807. doi:10.1155/2018/6463807